
|
|
Treatment Options and Restorative Materials
To help you make an informed decision regarding various treatment options, this page is devoted to providing you with the necessary information you will require. Restoring Teeth - materials options:
Replacing Teeth -Treatment options:
MATERIAL OPTIONS
ALL CERAMICS. Definitely the trend in dentistry as they provide optimal physical characteristics along with the aesthetic requirements of the patients. For simple crowns, onlays and inlays, we generally recommend the CEREC (Sirona, Bensheim, Germany) CAD/CAM system. Used by us since 1998, we have found this to give the highest clinical success and comfort to the patient. A very impressive system using optical scanning of your tooth, computer design and finally in-house computer robotic manufacture, we are able to deliver this restoration in one appointment. The success is largely due to the industrially manufactured ceramic which, along with being the most inert and biocompatible material used in dentistry, is due to the following factors:
Added bonuses to the patient include the time saved by not coming back for temporary recementation and final insertion as well as not having sensitivity during the temporary phase. In other instances, where CEREC may not be the optimal choice, we will then recommend other All Ceramic systems. These will generally be for bridges, veneers and anterior crowns. There are numerous systems that will be used, many of which will require some degree of CAD/CAM manufacture in their fabrication. Again, their advantages include the very highest degree of anterior aesthetics as well as strength where space age materials such as zirconia are used.  roll over image to reveal Cerec restorations
COMPOSITE. This is a tooth-coloured 'composition' of a resin matrix filled with inert glass particles. This popular restorative material is actually adhesively bonded to the available tooth surface, thereby reducing microleakage and actually increasing the strength of the available tooth. In smaller applications, this is an excellent material and gives an aesthetic appearance with very little tooth sensitivity. Its drawbacks come when filling larger cavities. Since it is a resin based material, curing results in polymerization shrinkage which can result in cracking of the tooth structure. In addition, it can be very hard to completely fill the available cavity, thereby allowing voids and leakage.
GOLD ALLOYS. For many years, this has been the 'gold standard' and is still an excellent material. Once placed, it can have a useful lifespan of more than thirty years. Its drawbacks are that it is generally cemented (as opposed to bonded) to your tooth structure and generally requires some additional tooth removal in order to physically anchor it to your tooth. Aside from frequent cold sensitivity (metal is an excellent thermal conductor) after placement, it is becoming less popular due its metal appearance. In some instances, especially where we cannot reliably bond to your tooth structure, it will be the recommended treatment. This will generally be in the very back of your mouth, i.e. the second molar region. 
METAL CERAMICS (a.k.a. Porcelain Fused to Metal or PFM). For years, a mainstay for crowning procedures, we are using it less and less due to the aggressive tooth removal required and the dark shadows along the gum lines. The metal core under the ceramic will inhibit light transmission and can lead to the unsightly black lines along your gum line as well as a dark appearance on the gum area. In some instances, especially where bonding cannot be done reliably, we will be recommending this material for cementation. 
AMALGAM. This is an 'amalgamation' of a variety of heavy metals, including mercury (about 50%), silver, tin, indium, copper and other trace substances. In the past, this has been one of the mainstay materials of dentistry and owes its success to its corrosion properties as well as the toxicity of the mercury to the bacteria. Failure occurs through leakage and decay as well as increased expansion over time resulting in tooth cracking/fractures. Although mercury fillings are not considered a problem in 99+% of humans, they will not be an option in our office. As significant mercury vapour is released during placement - and to some degree during removal - team members are exposed to repeated usage. Another major factor is environmental. Many European countries have banned Amalgam due to the mercury contamination of sewage once the fillings are removed. They tend to escape into the river systems, thereby affecting the fish in major estuaries. Naturally, this has become an environmental concern for the Fraser River Sturgeon and Salmon and, for this reason, we have acted on inevitable legislation and installed a mercury scavenging device in our clinic. For a nominal cost to us, we recycle the mercury waste to a certified waste removal company. 
TOOTH REPLACEMENT OPTIONS IMPLANTS. This is now considered the 'gold standard' of tooth replacement and is considered the closest thing we have to natural tooth replacement. Having a very high success rate (95+%), once integrated to your bone, this now maintains the bone as though you had your own tooth. It also takes the full load and obviates overloading of the adjacent teeth as with fixed bridges. Disadvantages to implants include perceived cost as well as time required until the final restoration. In some situations, it will require bone grafting which will add to the complexity and cost of treatment. 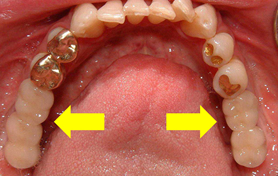 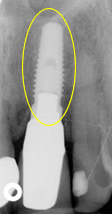
FIXED BRIDGES. Due to implant dentistry, this is no longer considered the optimal options that it once was. Utilizing adjacent teeth prepared (ground) to crown abutments, the bridge is then fixed by cementing to the abutment teeth. The result can be very aesthetic and functional allowing the patient to chew with full force and confidence. Its disadvantages include the necessity to remove healthy tooth structure from the neighbouring teeth as well as the extra force applied to the abutments. Unless used late in life, failure is eventual and can result in serious compromise to the abutment teeth. 
REMOVABLE PARTIAL DENTURES. In the situation where some teeth are present, this is a very useful system. Involving a metal strap or bar that either crosses your palate or goes under your tongue, these appliances are removed at any time. In situations where either implants or fixed bridges are not feasible, these can be very useful. Disadvantages include lack of patient acceptance, movement and food impaction during eating and the eventual reduction in the fit as time goes by. In the event, the metal clasps ('hooks') are considered unaesthetic, precision attachments can sometimes be used. 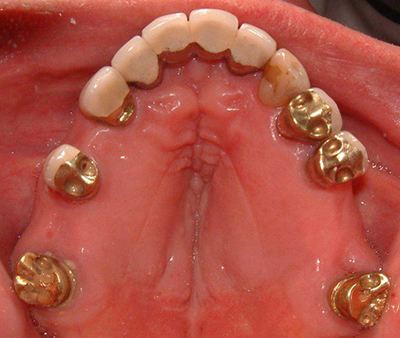 (roll over image to see removable partial denture)
NO TREATMENT. In some instances, especially in later life, this may be deemed the advised treatment. In the event that this is not the advised treatment and occurs when the patient neglects to replace missing teeth, shifting of the teeth will occur over the years and may require braces (orthodontic therapy) in the future when restoration is sought by the patient.
What are the right options for you? Please ask us if you have any questions. It may be that the treatments recommended by us may not be the options that will be chosen by you. Remember, its your decision.
|
||||||||||||||||||||||||
